A group from Cliniques universitaires Saint-Luc, Belgium, etc. has reported relationship between serum uric acid level and COVID-19 severity.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8201458/
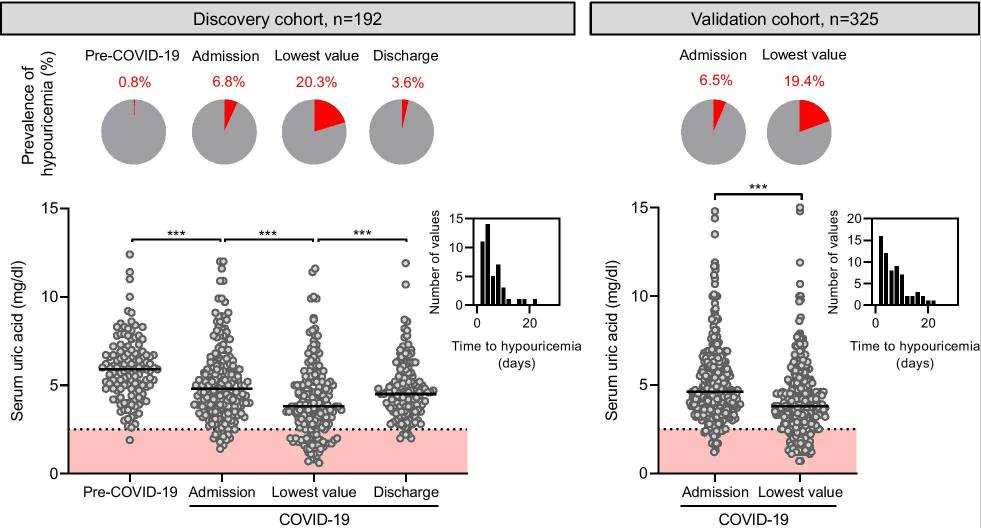
The prevalence of hypouricemia is approximately 0.3% in the general ambulatory population. In this study, 20% of the patients hospitalized for SARS-CoV-2 infection developed hypouricemia, a proportion that increased to 77% among patients requiring mechanical ventilation.
Uric acid is the end-product of purine metabolism in humans and is generated in the liver. The kidney is an important regulator of circulating uric acid levels as it excretes most of total body uric acid. Serum urate is freely filtered by the glomeruli followed by a complex balance of reabsorption and secretion in the kidney proximal tubule. Although the molecular mechanisms of urate transport in the proximal tubule are still incompletely understood, URAT1 (SLC22A12) is the main apical transporter mediating urate reabsorption in the brush border of the proximal tubule. In a small subset of kidney samples from patients who died from COVID-19, it was shown that life-threatening SARS-CoV-2 infection is associated with a significant (~ 70%) decrease in the expression of the apical urate transporter URAT1 in the kidney proximal tubule, contributing to the impaired tubular absorption of urate. The mechanisms linking hypouricemia and progression to severe disease requiring mechanical ventilation in patients with COVID-19 remains speculative and may be diverse
Anyhow, it seems that serum uric acid could be used as a reliable biomarker to identify patients at risk of life-threatening COVID-19.