A group from University of Oxford, etc. has reported quite interesting immune response of HIV infected children.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7763548/
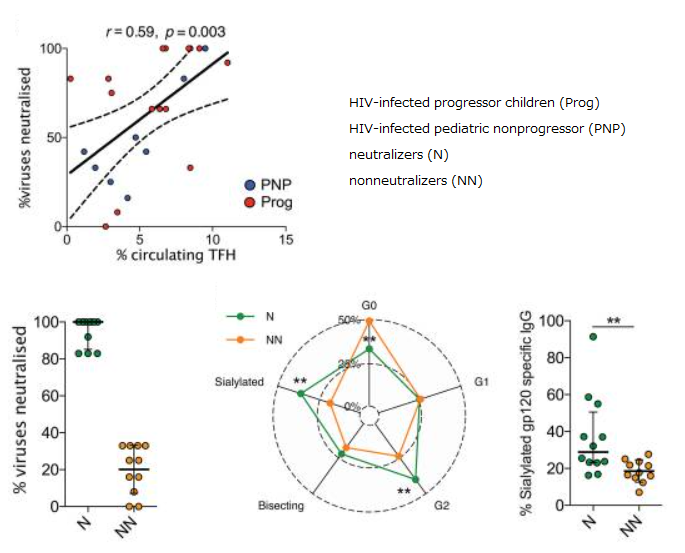
There are some asymptomatic children, HIV-infected pediatric nonprogressors (PNPs), who maintain normal CD4 counts HIV despite ongoing viral replication at high rates in the absence of antiretroviral therapy (ATR). It is also very interesting that some children develop broadly neutralizing antibodies (bnAb). It is also characteristic that the effector functions (ADCC and ADCP) mediated by IgG Fc binding to effector cells such as NK cells and macrophages are strong in the PNPs.
As for IgG glycosylation, PNPs have similar glycosylation to health controls, or rather, slightly higher sialylation and lower core fucosylation, although HIV infected adults usually develop agalacto type N-glycans.
It was also found that bnAb collelated with circulating Tfh cells and sialylation of gp120-specific IgG.
It is well know that the effector functions via IgG Fc binding get higher with increasing core fucosylation.
Taking these things into consideration, the immune activation in PNPs is rather low, but it might be compensated by the existence of bnAb and stronger effector functions.