A group from University of Liverpool has reported results of random forests model (one of machine learning methods) to predict the animal host of SARS-CoV-2.
https://journals.plos.org/plospathogens/article?id=10.1371/journal.ppat.1009149
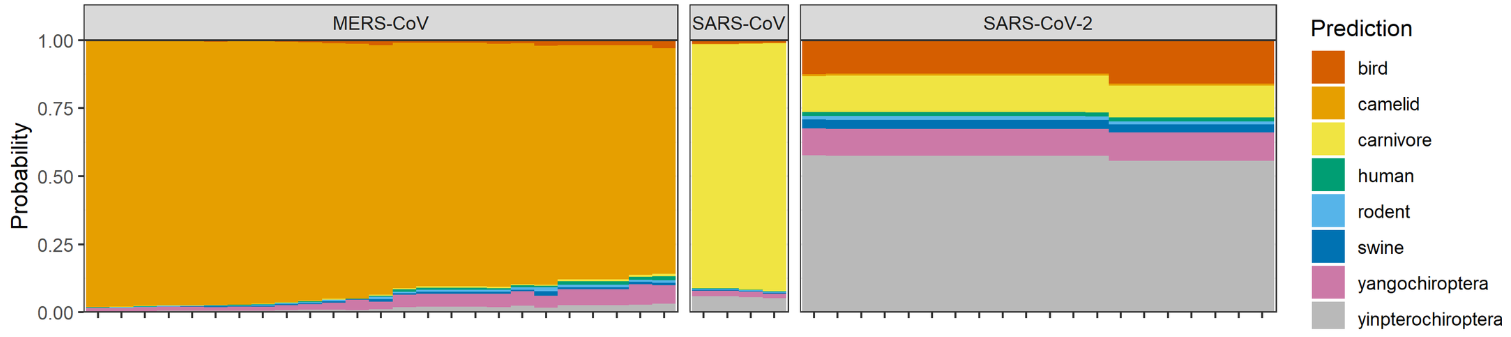
A figure below shows stacked bar plots of predicted probabilities of each host category for coronavirus RNA sequences, assuming bird, camelid, carnivore, human, rodent, swine, yangochiroptera, and yinpterochiroptera as potential hosts. It is clearly shown that MARS-CoV has camelid host, SARS-CoV has carnivore host, and SARS-CoV2 seems to have a bat host (suborder Yinpterochiroptera). While the random forests model supports bats as the ultimate origin of SARS-CoV-2, the involvement of intermediate hosts remains unclear.