Inhibition of C2GnT (O-glycan Core2 acetylglucosaminyltransferase)would be effective for the treatment of Choriocarcinoma
A group from Medical School, Nagoya University has reported that the inhibition of C2GnT (O-glycan Core2 acetylglucosaminyltransferase)would be effective for the treatment of choriocarcinoma.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7895715/
Choriocarcinoma is a disease specific to women and a malignant tumor produced in placental trophoblasts.
It was thought that cytotoxicity of NK cells is activated through interraction between NKG2D, which is a receptor expressed and on NK cells, and MHC class I-related chain A (MICA), which is often expressed on tumor cells.
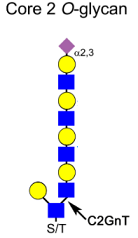
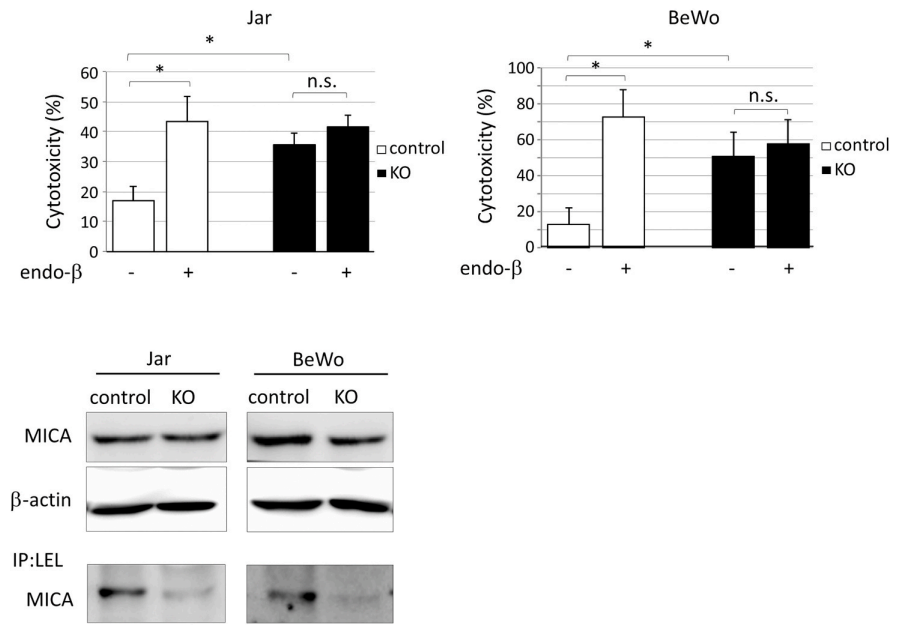
As shown in the figures below, it is obvious that MICA is O-glycosylated with a core 2 poly lactosamine elongated structure, because glyco-catched MICA with LEL lectin decreases with C2GnT KO. By knocking out C2GnT, the elongation of core 2 structures with poly lactosamine is prohibited, of course. Jar and BeWo are choriocarcinoma cell lines, and the comparison between control and C2GnT KO cells shows that NK cell cytotoxicity increases with C2GnT KO. And it is also clear that NK cell cytotoxicity is activated by endo-β-galactosidase treatment, because it cut out poly lactosamine structures from core 2 O-glycans.
So, these results indicate that poly lactosamine elongation of core2 O-glycan is inhibiting NK cell cytotoxicity, and therefore, with increasing C2GnT, choriocarcinoma cells could escape from NK cell attacks eventually. This also means that inhibition of C2GnT would be effective for the treatment of choriocarcinoma.