A group from the University of Florida etc. has found that people with vitamin D deficiency were five times more likely to be infected with COVID-19 than people without deficiency after adjusting for age groups (OR = 5.155; 95%CI、3.974–6.688; P <0.001)from a statistical study using total population of 987,849 people. Healthy diets is the base of health. Sorry for the very short blog article.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7716744/
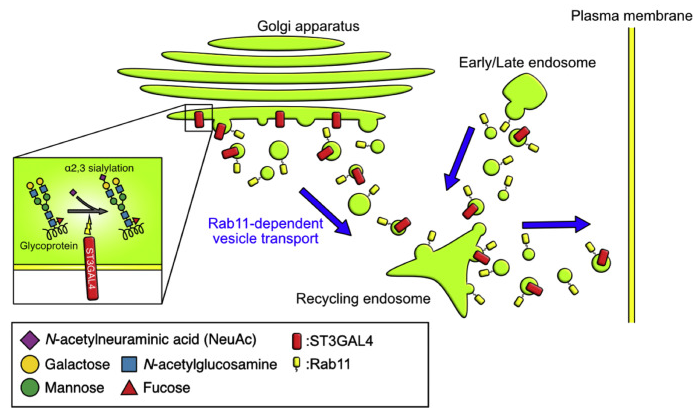
How is Rab11 (a regulator of membrane vesicle transport via recycling endosomes) related to N-glycan modification?
A group from Osaka University etc. has found that Rab11 (a regulator of membrane vesicle transport via recycling endosomes) is deeply involved in N-glycan modification.
https://www.jbc.org/article/S0021-9258(21)00126-5/fulltext
Glycan modification is controlled by glycosyltransferases present in the endoplasmic reticulum and Golgi bodies. Therefore, if each glycosyltransferase is not in an appropriate position, the glycan modification is not performed correctly. Unfortunately, the mechanism for transporting glycosyltransferases to the correct positions is not known.
The authors have found that Rab11, a regulator of membrane vesicle transport, was heavily involved in the modification of α2-3Sia. In cells that knocked out Rab11, the modification of α2-3Sia was greatly upregulated, and thereby it was found that Rab11 negatively controlled the α2-3Sia modification by transporting the glycosyltransferase ST3GAL4 out of the Golgi body region.
The figure below shows the role of Rab11 in a healthy state.
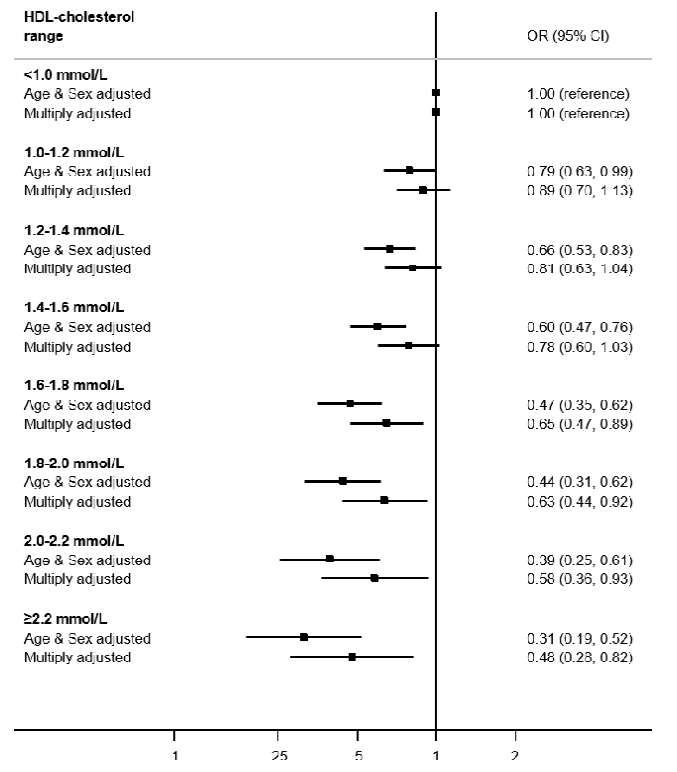
High HDL good cholesterol greatly reduces risk of infection with the new coronavirus (SARS-CoV-2)
A group from The Hospital del Mar Medical Research Institute (IMIM), Barcelona, Spain etc. has reported that high HDL good cholesterol significantly reduces the risk of covid-19 infection.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7852244/
As shown in the figure below, it can be shown that as HDL cholesterol increases, the risk of infection with the new coronavirus (SARS-CoV-2) is reduced monotonically. The statistical analysis was performed with data from 317,306 people. By multiplying 38.66535, mmol/L can be converted to mg/dL.
Relationship between a pro-thrombotic platelet phenotype (P-Selectin, GPIIb/IIIa complex etc.) and the new coronavirus (COVID-19)
The new coronavirus (Covid-19) is known to cause a hypercoagulable state such as cardiovascular complications as well as acute respiratory distress syndrome (ARDS).
A group from Technical University of Munich etc. has used antibody panels of 21 membrane-penetrating proteins, to investigate the expression status of those markers in platelets by mass cytometry.
https://www.nature.com/articles/s41419-020-03333-9
From Mass cytometry, it was fount that the expression of P-Selectin (0.67 vs. 1.87 Healthy Median vs. Median COVID-19 patients, p = 0.0015), LAMP-3 (CD63, 0.37 vs. 0.81, p = 0.0004), GPIIb/IIIa complex (4.58 vs. 5.03, p< 0.0001) are upregulated. P-Selectin functions as a cell adhesion molecule on the surfaces of activated endothelial cells, which line the inner surface of blood vessels, and activates platelets. GPIIb/IIIa is an integrin complex found on platelets, a receptor for fibrinogen and von Willebrand factor, and aids platelet activation。LAMP-3 is one of the lysosome-associated membrane glycoproteins。
The adhesion protein P-Selectin translocates to the plasma membrane upon activation and regulates platelet–leukocyte interactions resulting in activation of neutrophil integrins and inducing NETS formation. NETS is one of functions of innate immunity, and capture and eliminate virus. However, the excess NETS leads to hypercoagulopathy. P-Selectin expression together with the upregulation of the GPIIb/IIIa comples contributes to the COVID-19 inflammatory response. Although the pathophysiological mechanisms behind the high incidence of thromboembolic events in hospitalized COVID-19 patients remain unclear and the key drivers behind platelet activation in COVID-19 remain to be determined, it may be induced by infected endothelium as well as by the cytokine storm occurring during SARS-CoV-2 infection.
The new coronavirus (SARS-CoV-2) and ABO Blood Types
Several research institutes have already reported that type O blood is more resistant to SARS-CoV-2 and type A blood is less resistant. This suggests that the presence of anti-A antibodies must be related to SARS-CoV-2 infection protection.
A group from Universe libre de Bruxelles (ULB), Brussels, Belgium, etc. has speculated that the presence of anti-A and anti-B antibodies is a true problem and that it is related to the protective effect against SARS-CoV-2.
https://www.ijidonline.com/article/S1201-9712(20)32549-2/fulltext
Type O: IgM anti-A+ anti-B agglutination score: 88.29±33.01 (healthy people), 76.93±34.93 (COVID-19 patients)
Type A: IgM Anti-B agglutination score: 30.40±18.84 (Healthy), 24.93±18.73 (COVID-19 Patients)
Type B: IgM anti-A agglutination score: 36.50±17.41 (healthy persons), 28.56±17.41 (COVID-19 patients)
From these results, it could be said that as the presence of anti-A antibodies and anti-B antibodies is small, the resistance to SARS-CoV-2 weakens and it becomes easy to become infected, and if the amount of presence is not large, the effect of infection protection due to differences in blood types would not be clear.
Anti-A and anti-B antibodies are synthesized by immune stimulation from gastrointestinal microbiota. Both these antibody production and microbiota vary greatly according to an individual’s age and nutritional status. In other words, the promotion of ABO antibody production by the gastrointestinal microbiota will help prevent the infection of the novel coronavirus! ?
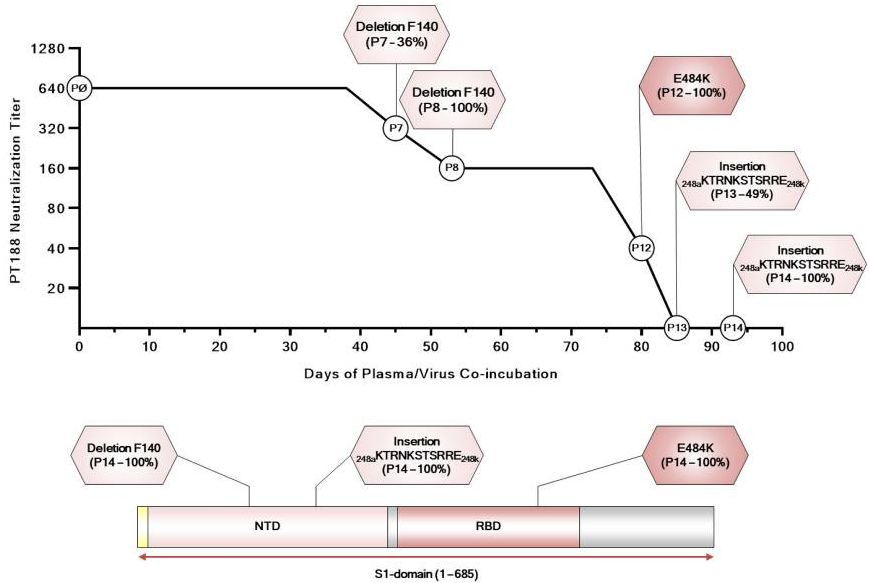
Plasma neutralizing antibodies in convalescent patients recovering from the new coronavirus (COVID-19) stop working with time
The key question in vaccine development would be, under the selective pressure of the polyclonal immune response of vaccinated people, if the virus evolves to escape from the immunity? and if it is effective against virus mutations or not?
A group from Fondazione Toscana Life Sciences, Siena, Italy etc. has reported the results of co-culture of cells and virus with using neutralize antibodies (polyclonal) obtained from the plasma of convalescent patients from the new coronavirus (COVID-19).
https://pubmed.ncbi.nlm.nih.gov/33398278/
In this experiment, VERO E6 cells and SARS-CoV-2 were co-cultured for 100 days (14 passages over) using neutralizing antibodies with the highest neutralizing titer among 20 convalescent patients, to investigate the relationship between changes in the titer of neutralize antibodies and genetic mutations that occurred in viruses. In this experiment, the following mutations have occurred in the NTD and RBD of the S protein, and it is shown that the titer of the neutralize antibody decreases with it.
- deletion of the phenylalanine in position 140 (F140) on the S-protein NTD N3 loop.
- glutamic acid in position 484 of the RBD was substituted with a lysine (E484K).
- 11-amino-acid insertion between Y248 and L249 in the NTD N5 loop (248aKTRNKSTSRRE248k).
The results of this experiment show that virus can evolve to escape from the selective pressure of even the highest titer neutralize antibodies. So, it is recommended to use cocktail antibodies for treatment. In addition, it suggests the need to develop a second-generation vaccine that can accommodate mutations.
Genetic variants in Mannose Binding Lectin (MBL) appears to be significantly related to the severity of the new coronavirus (COVID-19)
It is known that there are three type of innate immunity, (1)phagocytosis with phagocytic cells such as macrophages and NK cells, (2)complement lectin pathways, and (3)extra-spherical traps . In the complement lectin pathway, Mannose Binding Lectin (MBL) plays a central role, and when MBL binds to the mannose on the pathogen’s cell membrane, an enzyme called MBL-binding serine protease (MASP) bound to MBL is activated, and MASP activates the complement Factor 4 (C4), which sequentially activates the complements and ultimately kills it by drilling a hole in the pathogen’s cell membrane.
A group of Istanbul Faculty of Medicine, Istanbul Univ. has reported that the genetic variants in MBL are largely related to the severity of covid-19.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7838598/
For the mutation of codon52 of the MBL2 gene,
Referring to AA genotype,
BB genotype: odds ratio (OR) = 5.3, p< 0.001;
AB genotype: OR = 2.9, p = 0.001
For the ICU need, the odds ratios get higher as follows,
BB genotype: OR = 19.6, p < 0.001
AB genotype: OR = 6.9, p = 0.001
This could be a good reference in using MBL as a therapeutic protein.
Importance of Innate Lymphoid Cells (ILCs) in the new coronavirus (COVID-19)
The new coronavirus (COVID-19) causes lymphopenia. However, an interesting fact emerges when the correlation with the disease severity is examined in detail about the subsets of the lymphocytes.
A group from The University of Massachusetts Medical School etc. has focused on Innate Lymphoid Cells (ILCs) and reported an interesting correlation with the severity of COVID-19.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7814851/
ILCs are lymphocytes that do not have antigen receptors and are the main biological defense mechanism in immunity in the prestage leading up to the development of acquired immunity. NK cells with cytotoxicity are also classified as ILCs. It can be said that ILCs are divided into those mainly producing cytokines and those with cytotoxicity. In this paper, ILCs are defined as cell populations excluding NK cells.
In patients with COVID-19, ILCs are reduced by 1.78 times (95% CI: 2.34–1.36) and CD16+ NK cells by 2.31 times (95% CI: 3.1–1.71) compared to healthy people.
Interestingly, it was shown that ILCs was, but not CD16+ NK cells, CD4+ T cells, or CD8+ T cells, correlated with hospitalization, and the odds ratio of hospitalization was 0.413 (95% CI: 0.197–0.724) for every 2-fold increase in ILCs. They also showed that as ILCs increased, the odds ratio of hospitalization rates decreased, duration of hospitalization were shortened, and CRP, an inflammatory marker, decreased.
This finding is likely to lead to new treatments, I feel.
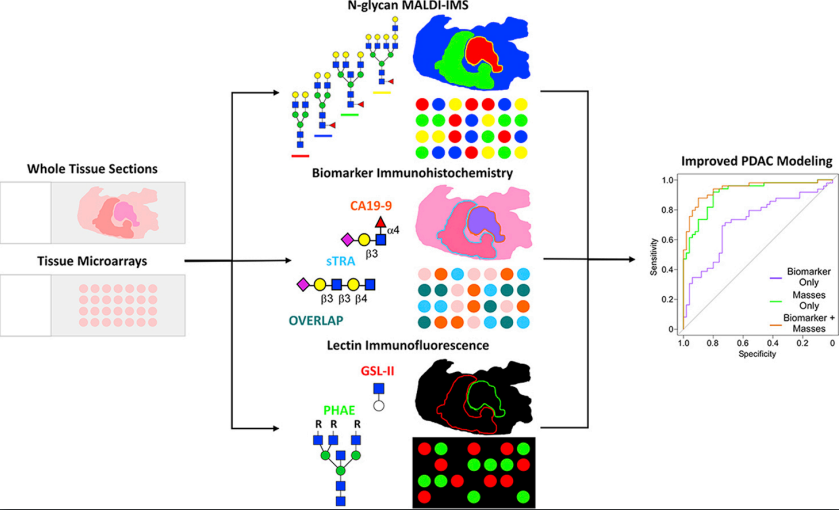
Glycan markers for pancreatic duct adenocarcinoma
A group from Medical University of South Carolina etc. has reported their findings on glycan markers for pancreatic duct adenocarcinoma.
https://www.mcponline.org/article/S1535-9476(20)35126-4/fulltext
In order to study the glycan markers of pancreatic duct adenocarcinoma in detail, MS (MALDI-FTICR, MALDI-QTOF), antibody immunostaining (CA19-9, TRA-1-60), lectin staining (PHA-E, GSL-II) were used.
To summarize the results, pancreatic duct adenocarcinoma has an increase in the structure of α2-3 Sia, poly-LacNAc, branching, bisecting GlcNAc, core fucose, and terminal GalNAc compared to normal tissues. As for Sia, α2-3Sia is mainly expressed in tumor stroma regions, and α2-6Sia is slightly stronger in adenocarcinoma regions.
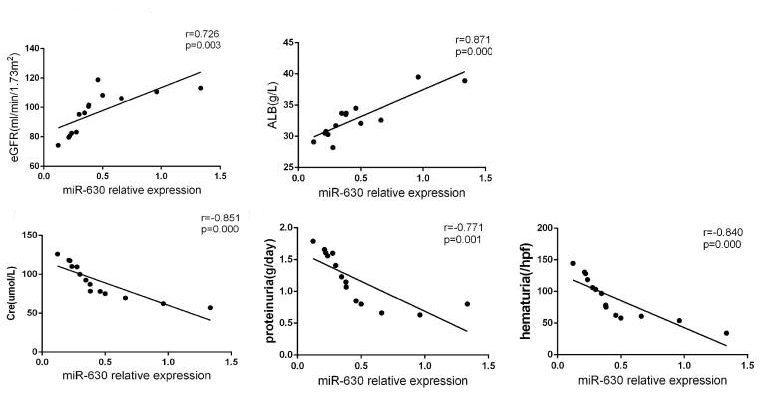
MicroRNA (miR-630) derived from tonsils may be deeply involved in IgA nephropathy
IgA nephropathy is a typical intractable disease of chronic kidney disease in which IgA (one of the immunoglobulins) is deposited in the glomerulus (a urine filtration device) with aberrant glycan modification. It is also well known that abnormalities occur in the O-glycan modification in the IgA hinge region.
A group from Central South University, Changsha, China etc. has indicated that IgA, the glycan abnormality found in IgA nephropathy, might be controlled by microRNA (miR-630) derived from tonsil mononucleated cells.
https://www.frontiersin.org/articles/10.3389/fimmu.2020.563699/full
As for the mechanism of the onset of IgA nephropathy, it was suggested that miR-630 derived from the tonsils is produced excessively, and targets Toll-like receptor 4 (TLR4) as the target gene, and finally modulates the concentration of IgA and its glycosylation level through the NF-kB signaling pathway.