A group from Fukushima Medical University has discussed about a key-point on colorectal cancer immunotherapy based on colorectal cancer and Tn-antigen.
https://www.mdpi.com/1422-0067/21/23/9081
In cancer, mutations are accumulated in the genome and epigenome. In colorectal cancer, 85% are derived from chromosomal instability and 15% from deficient mismatch-repair (dMMR).
It is also well known that in cancer, aberrant glycans are expressed on the cell surface, and O-type glycans are truncated, and resulting Tn-antigens are highly expressed. Tn-antigen binds to macrophage MGL and promotes il-10 secretion and acts immuno-suppressively, as well as inducing T-cell apoptosis. As a result, cancer cells evade immunity attacks.
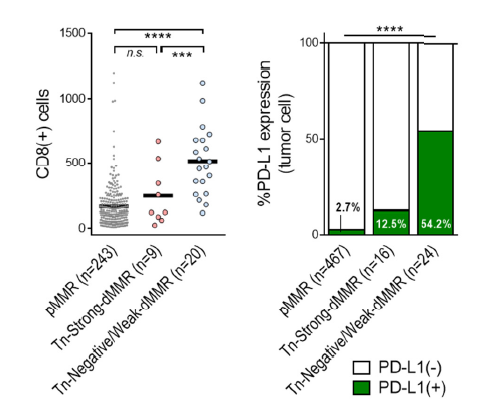
Cancer cells with deficient mismatch-repair have significantly higher expression of Tn-antigen than those that are not. In addition, those types of cancer cells tend to have less infiltration of CD8+ T-cells and lower expression of PD-L1 as an immune checkpoint molecule. Therefore, they have concluded that immunotherapy targeting on Tn-antigens and inhibition of immune checkpoint molecules may be effective for colorectal cancer with a strong deficient mismatch-repair.