A group from Oklahoma Medical Research Foundation, Oklahoma, USA, etc. has reported that L-SIGN is a receptor for authentic SARS-CoV-2 infection.
https://insight.jci.org/articles/view/148999
To examine if L-SIGN interacts with SARS-CoV-2, lentivirus-based SARS-CoV-2 pseudo-typed virus (CoV-2–type virus) and HEK293T cell lines expressing L-SIGN-flag or ACE2-myc3 as positive control were established. L-SIGN is a C-type lectin which binds to high-mannose–type N-glycan and Ca2+ dependent manner. The RBD of the SARS-CoV-2 spike protein has an N-glycosylation site at Asn343. N-glycan–deficient spike/Fc, in which Asn343 was replaced with glutamine (Q) (SpikeN343Q/Fc) was developed, and the mannose moiety deficiency on SpikeN343Q/Fc were confirmed by mannose-specific GNL blotting. Thus, it was confirmed as shown below that SpikeN343Q/Fc binds to cells expressing ACE2 but not to cells expressing L-SIGN, indicating that L-SIGN recognizes an N-glycan structure on Asn343.

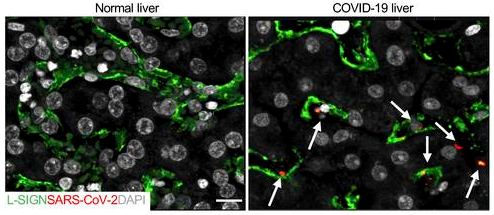
L-SIGN but not ACE2 is uniquely expressed on human liver sinusoidal endothelial cells (LSECs). To determine the clinical significance of the interaction between SARS-CoV-2 and L-SIGN, it was first examined if SARS-CoV-2 was present in LSECs from formalin-fixed paraffin-embedded liver autopsy samples from patients with COVID-19. In comparison with uninfected human liver autopsy samples, SARS-CoV-2 was detected with an anti-SARS-CoV-2 nucleocapsid antibody inside patient LSECs as shown below (LSECs were L-SIGN+ (green)and arrows mark SARS-CoV-2 (red)).
In addition, it was shown that SARS-CoV-2 infection was blocked with an antibody against human L-SIGN and also with mannan dose-dependently, suggesting these could be potential therapeutic options to treat severe COVID-19 infection.