A group from Icahn School of Medicine at Mount Sinai, New York, USA, etc. has reported on characteristics of Pfizer mRNA vaccinated SARS-CoV-2 antibodies.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8185186/
The antibody response peaked 1 week after the second vaccine dose, followed by a decline in titers over the following weeks as expected from an antibody response to vaccination. Interestingly, titers against the spike proteins of β-coronaviruses OC43 and HKU1 increased substantially after vaccination.
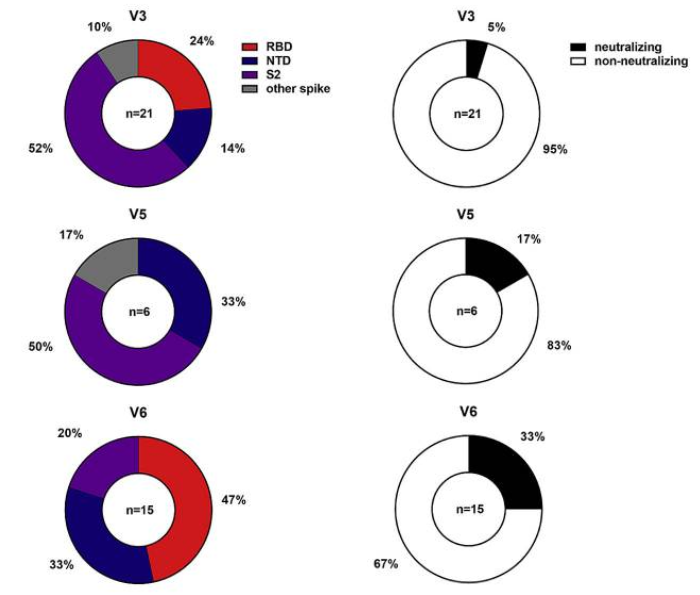
RBD and NTD were co-dominant epitopes of the mRNA vaccine-induced antibodies, and the majority of remaining epitopes was mapped to S2. All antibodies were tested for neutralizing activity against the USA-WA1/2020 strain of SARS-CoV-2. Only a minority of the binding antibodies showed neutralizing activity (see figure below, obtained from three individuals: V1, V5, V6).
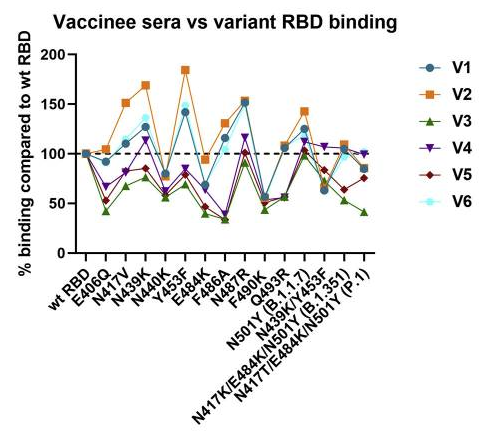
For sera from the six vaccinated individuals, binding between vaccinee sera and variant RBDs were evaluated. The highest reduction was only 2-fold for E406Q, N440K, E484K, and F490K (see figure below, six vaccinated individuals: V1-V6).
This would be a kind of good news showing that Pfizer mRNA vaccine would be effective against current SARS-CoV-2 variants.